The case study that we have described is based upon data and discussions from Mozambique, but there are ways to adapt segmentations to be used more widely across different geographies. Before implementing either of these sets of interventions and tools, consider how well they might apply to your local context.
First, there must be interest in implementing interventions on the part of the Ministry of Health counterparts working in nutrition. Then, the existing segmentation should be reviewed in detail with local nutrition stakeholders to determine if the segmentation seems relevant for the local context. This step assesses if the factors influencing segment behaviors resonate with nutrition stakeholders. If many or all of the characteristics of the segmentation are applicable and there is a desire to see if additional country-specific factors arise, then qualitative research may be helpful. For example, conducting focus groups or individual interviews, utilizing the segment identification tool as a screener. After the segmentation has been sufficiently adapted, locally relevant recommendations can be developed and implemented.
Note that if very few of the segments resonate with local stakeholders, it might be necessary to conduct an entirely new segmentation (following the steps outlined in session 2 and 3 of this course).
Please see the description below for more detailed instructions. Click each step to learn how to adapt segmentation findings and interventions for local contexts.
Step 1. Bring together nutrition stakeholders
Step 1
Identify and bring together nutrition stakeholders to discuss how this segmentation applies to the local context and determine interest in piloting an intervention.
Description
To assess the relevance of these segments in your country, share the chosen segmentation with the following entities to gather their inputs based on their experience in the country.
Ministry of health officials
Nutrition professionals and health care providers
Local Implementing partners
This step assesses if the factors influencing segment behaviors resonate with teams working on nutrition in the country.
Step 2. Explore country-specific nuances through qualitative research
Step 2
If possible, explore country-specific nuances through qualitative research.
Use the segment identification tool as a screener to identify individuals from the population for focus groups and in-depth interviews across each segment.
Analyze the outputs of the focus groups and identify common themes between the segmentation and any country-specific factors.
Adjust the segment personas and intervention recommendations to better reflect the local research findings.
Description
Conducting qualitative research is an important step before using the segmentation to confirm the factors influencing each segment behavior and uncover any country-specific factors.
Check if obtaining ethics approval for the research will be required.
Develop discussion guides for the research, including the topics that may be different in the local context.
Recruit individuals across each segment using the segment identification tool as a screener.
Conduct dedicated focus groups or individual interviews and use the discussion guides to test if the factors driving the segment’s behavior are similar in the local context and explore if other factors exist.
Update each segment persona and reflect these nuanced factors in the segment recommendations.
Step 3. Roll out
Step 3
Once a locally relevant intervention has been designed based on the discussions and qualitative research, it should be rolled out within Health Facilities, Communities, or Training Centers, depending on the intervention selected.
Description
Once the segmentation and intervention design has been updated to reflect the local context, the intervention can be rolled out using the following steps:
If needed, translate the tools into the local language(s) for each geography to ensure it is accessible.
From there, pretest the intervention with 6-10 individuals of the community of interest (e.g., clients or providers) to collect feedback and identify gaps.
Following the pretest, pilot the intervention for 3-6 months.
Before launching the pilot, it is critical to define a monitoring and evaluation framework and a training process to introduce the tools. The intervention should ideally be embedded in existing processes. During the pilot phase, supervision is needed to assess the intervention through frequent feedback and discussion.
If successful, consider scaling the tool for use in additional locations in the larger geographic zone based on the results of the pilot.
Key Takeaways
It is important to collaborate with a diverse team of stakeholders to develop SBC solutions that are engaging, relevant, and impactful.
When piloting the intervention, make sure to assign roles and responsibilities for the intervention to the appropriate parties. It is critical to include training, monitoring, and evaluation strategies that ensure a smooth implementation of the pilot, enable an understanding of how to refine and improve the tool, and assess the effectiveness of the intervention for potential scale-up.
It is vital to adapt the interventions for use in local contexts. To do so, review the segmentation analyses and tools with local stakeholders and involve the target population in determining what additional contextual findings can be added to the segmentation analyses and interventions presented here.
Check Your Understanding
Thank you for completing the third session of Audience Segmentation for Nutrition Next is an ungraded quiz to test your understanding of Session 3. Click the Knowledge Check button to get started.
https://learning.breakthroughactionandresearch.org/wp-content/uploads/BA-logo-horizontal-300x110.png00Carriehttps://learning.breakthroughactionandresearch.org/wp-content/uploads/BA-logo-horizontal-300x110.pngCarrie2024-01-12 06:03:062024-02-08 12:30:26Adapting the Tools
The purpose of this session is to describe the steps of conducting audience segmentation in more detail and provide an example, or case study, of a segmentation effort developed to inform nutrition SBC programming. The case study is a nutrition segmentation analysis conducted among pregnant and postpartum women in Mozambique. Session 3 will cover interventions and recommendations for the case study.
Learning Objectives
List the steps and resources required to conduct an audience segmentation with a quantitative foundation and complementary qualitative research.
Describe a psychosocial segmentation conducted among pregnant and postpartum women in Mozambique.
List key distinguishing factors of each segment.
Describe a tool to segment members of a target population to tailor SBC interventions.
Steps to Create a Segmentation
Session 1 introduced the concept of audience segmentation, defined types of segmentation, described the role of audience segmentation in nutrition SBC, and outlined the steps required to conduct an audience segmentation. This session will describe the first seven steps required to conduct an audience segmentation in greater detail. (Steps 8-11 are covered in Session 3.)
Identify the priority behaviors
Define the target population
Enlist key stakeholders
Develop research questions
Select a dataset
Define segments
Refine your segments
Develop intervention elements
Pilot solution
Evaluate & Refine
Adapt & Scale
Step 1. Identify the Priority Behaviors
Audience segmentation provides great insight into how certain behaviors vary across a population and can be used to identify and prioritize groups for social and behavior change. To leverage audience segmentation, start by identifying the priority behaviors. For example, which nutrition-related behavior needs to be addressed in your local context? What is the desired behavior change that will result in improving nutrition outcomes?
Below are some examples of nutrition priorities. Use these as a starting point for brainstorming the desired social or behavior change for your segmentation.
Consumption of the recommended number of food groups per day
Providing recommended number of food groups per day to one’s child
Providing recommended quantity of food to one’s child per day
Seeking nutrition related advice from a health care worker
Step 2. Define the Target Population
Second, determine which population you want to encourage the desired behavior change within. Looking at DHS data, for example, we can determine which populations may be particularly vulnerable to issues related to nutrition. Examples of populations of interest to focus on nutrition behavior change include pregnant women, caregivers of children under 5, health providers, and more.
Step 3. Enlist Key Stakeholders
Next, identify the individuals who should be involved in the segmentation effort, including those who may be required to conduct research and the segmentation analyses. It is important that stakeholders are aligned to the objective of the audience segmentation identified in steps 1 and 2, as they will be closely involved at different points in the process.
It is important to include a mix of stakeholders in the process, ensuring that they have an equal voice in providing feedback and decision-making. Ensuring a diversity of voices in the decision-making process is vital to designing inclusive solutions as they have direct impacts on people’s lives. Flip the functional group cards below to reveal their potential roles. Consider the functions that already exist on your own team, then fill in the gaps.
Knowledge
People with knowledge of national nutrition trends, data analysis, or primary data collection. Examples may include researchers, statisticians, or nutrition experts.
Experience
People with experience with in-country nutrition programs or in implementation and evaluation of interventions. Examples may include program implementers, staff from NGOs, or health personnel working directly with the population of interest.
Influence
People with influence over policy and quality improvement efforts for health facilities or at the health system level. Examples may include policy makers or Ministry of Health officials.
Step 4. Develop Research Questions
It is now time to develop the research questions to guide your audience segmentation. With your team, particularly those knowledgeable about national nutrition trends, determine the main factors related to the priority behavior that you want to better understand. It is helpful to conduct a search for peer-reviewed published articles and papers written on behaviors, beliefs, and attitudes towards nutrition in your country to ensure your research questions are not duplicative and are driven by existing data of what is already known. Consider the following:
Which factors influence the target population’s practice of nutrition-related behaviors? (e.g. what beliefs might they have about the behavior? What are the social norms related to the behavior? How are decisions made with respect to this behavior? Who might be influencing the target population? Where and how are they receiving information regarding this behavior?)
Among members of the target population, what are the characteristics of the individuals who are most likely to practice the priority nutrition-related behavior? What are the characteristics of the individuals who are least likely to practice the priority nutrition-related behavior?
How can the factors that influence the target population’s practice of the priority nutrition-related behavior be addressed through SBC interventions?
What is the likelihood that a member of the target population will adopt the practice of the priority nutrition-related behavior? What factors influence this likelihood?
Step 5. Select a Dataset
To conduct an audience segmentation using quantitative techniques, a survey dataset is required. At a minimum, this dataset should have the following parameters:
Come from a fairly recent survey, administered in the last 1-10 years, with a representative sample of the target population.
Report data for each survey respondent individually, not in aggregate.
Contain data on individuals in the specific population identified in step 2 (i.e., age, gender, occupation, etc.).
Contain variables that can be used as proxies for the outcome variables identified in step 4.
Contain data on the factors that influence the practice of the priority nutrition-related behavior among members of the target population.
Because segmentation is intended to describe segments and identify the drivers or influencers of behavior, your chosen dataset should also contain variables that are related to the outcome variables you identified in step 4. The list below contains examples of variables that your chosen dataset may include. Each type of variable has a different purpose for your audience segmentation dataset.
Demographic Factors
Characteristics of a population that would typically be collected in a census survey (e.g. age, gender, location, marital status, number of children, etc.).
Behavioral Factors
Observed or self-reported behaviors related to the priority health behavior (e.g. food consumption, or health seeking behaviors).
Attitudinal Factors
A way of thinking or feeling about someone or something, that is sometimes reflected in a person’s behavior. These can include perception of social norms, beliefs regarding a particular topic, and perception of one’s own personal agency over the behavior.
For nutrition, you may consider exploring the Demographic & Health Surveys (DHS) datasets to see if they would work for your audience segmentation.
Types of variables that may be present in datasets
Demographic
Use case
Best for simple segmentation or when combined with other variables as an additional descriptor.
Example characteristics
Age, location, gender, religion, number of children, rural/urban, literacy/numeracy, socio-economic status, household income, level of education, employment status or type, health history/risk factors, marriage status, etc.
Behavioral
Use case
Helpful for determining group actions and behaviors. Best when combined with attitudinal variables.
Example characteristics
Seeks information through specific channels, uses social media, goes to health center for illness or for preventive treatment, seeks care with traditional practitioners, involved in community activities, etc.
Attitudinal
Use case
Use when trying to understand rationale for behaviors. Best when combined with behavioral variables.
Example characteristics
Trust in authority (government, health institutions, health care professionals) and perceived: access to resources, perception of social norms (e.g., believes others practice certain health behaviors or not), role of fate/divine will, etc.
Step 6. Define Segments
At this point, it is time to analyze the data and define the segments. Quantitative segmentation analysis occurs in a 4-step process, which is described in greater detail below. Click each step to learn more about the process. It may be helpful to partner with your national statistical institute or a research firm to conduct these analyses.
1. Identify factors that are the main influencers or drivers of the research questions.
Step 1
Run a Chi-squared correlation analysis to identify which variables show a strong correlation with your priority behavior. This can help to test some of the hypotheses developed in step 4 (for example, women who believe in Y are more likely to do Z) After running these analyses on all of the variables in your dataset, identify the variables which showed the strongest correlation with your priority behavior.
2. Conduct a quantitative segmentation analysis and identify opportunities for positive behavior change.
Step 2
Analyze the variables identified in the previous step using one of the standard statistical methods for segmentation, which include cluster analysis and latent class analysis. These techniques help identify commonalities and trends among groups based on the variables in the data and selected outcome variables. This analysis will produce different options of segments in your dataset.
3. Review each segmentation model and determine the final model.
Step 3
Review model results of the segments identified in your dataset. Use the Bayesian information Criterion (BiC) indicator, to determine which models are statistically significant, with a lower BiC indicating a better model. Additionally, try and aim for a model with three to six segments so that it will be practical to implement. Finally, consider other factors to choose the best model:
How do the outcome variables and drivers of the outcome variables differ between various groups? Are the segments different enough from each other with regards to these variables?
Does the model tell a strong story about different groups within the population and their attitudes, behaviors, and beliefs around nutrition?
Are there any datapoints which are confusing and need to be further clarified and better understood? If so, change the active variables in your segmentation and re-run the models until everything is clear and the segmentation is quantitatively robust and easily understood.
4. Write a segment “persona” for each segment in the final model.
Step 4
Once a viable segmentation has been chosen, write a “persona” for each segment that describes the key distinguishing characteristics of the segment identified in analysis. Choose a name for each segment as well. The descriptive personas should be brief and easily digestible for dissemination and feedback. It primarily describes the segment in terms of the outcome variables and/or drivers of outcome variables.
Step 7. Refine Your Segments
The segments identified through quantitative analysis can be further refined using qualitative data collection and by speaking directly with individuals from each segment to gather additional information about the factors that shape the behaviors most characteristic of their segment.
Segment Identification Questionnaire
First, use a segment identification questionnaire to determine how to categorize individuals in the target population into the different segments. This will enable you to recruit individuals to participate in interviews, focus groups, or workshops for their segment.
A segment identification questionnaire can be developed using a Chi-squared automatic interaction detector (CHAID) algorithm in the R Studio orSPSS programs. This algorithm considers each variable used in the segmentation analysis as well as the final determined segments and identifies the variables that were most influential in forming the segments. This set of statistically significant variables may be asked in a brief survey to members of the target population to determine which segment they belong to.
Complementary Qualitative Research
Finally, if possible conduct qualitative research with members of each segment to develop a more comprehensive understanding of their behavioral drivers. Note that this will likely require some level of ethics approval, such as submitting a protocol to a local IRB (International Review Board) if you plan on interviewing vulnerable populations, asking sensitive questions, and / or plan on publishing the findings at a later date. Using the segment identification tool, invite members of the target population to participate in segment-specific focus groups or one-on-one interviews about behaviors and attitudes surrounding the priority behavior. Consider partnering with a local research firm to recruit participants, facilitate the interviews or focus groups, and analyze the findings. Aim to have 5-15 research participants for each segment.
Segmentation of Pregnant and Postpartum Women in Mozambique
Now, let us put segmentation steps 1-7 into practice with the case study example in the next lesson.
Segmentation of Pregnant and Postpartum Women in Mozambique
Case Study
In Mozambique, low rates of exclusive breastfeeding, limited vitamin intake, high rates of anemia among pregnant women and a predominantly starch-based diet have resulted in an estimated 1 in 2 children being nutritionally deficient (Lusambili, et al., 2020). Nearly a quarter of the population in Mozambique experiences food insecurity with agricultural production often in flux due to seasonality and various natural disasters. Seasonality is a large contributor to food shortages as the country goes through a ‘dry season’ where limited rainfall makes it difficult to produce crops at a rate that meets demand (World Food Programme, 2023).
Working alongside these systemic factors are various norms, beliefs, and practices that present barriers to achieving a diverse diet that offers the necessary vitamins and nutrients to keep mothers and children healthy.
Factors such as intergenerational food norms (beliefs or expectations on food preparation passed down by grandmothers and mothers-in law), societal taboos that dictate foods that should or should not be eaten during pregnancy or lactation, and gender dynamics that influence food allocation, health seeking, and task sharing all play a role in the dietary diversity of women and their children and affect their ability to obtain, prepare, and eat sufficient nutrient-rich foods in meals and snacks throughout the day (Lusambili et al., 2020). It is critical to understand and address the underlying factors driving decision-making around dietary diversity, both those within and outside of individual control.
This case study reviews a nutrition segmentation analysis that considered the factors driving dietary diversity among pregnant women and mothers to children under 2 in Mozambique. The insights presented in this session serve as the foundation for tailored interventions and recommendations that were developed for each segment presented in Session 3.
Sources
Lusambili, A., Naanyu, V., Manda, G., Mossman, L., Wisofschi, S., Pell, R., Jadavji, S., Obure, J., & Temmerman, M. (2020). Nutritional influences on the health of women and children in Cabo Delgado, Mozambique: A qualitative study. International Journal of Environmental Research and Public Health, 17(17), 6205. https://doi.org/10.3390/ijerph17176205
Given the above context, the priority nutritional behavior of dietary diversity was identified. Building from previous research conducted and USAID recommendations, dietary diversity was defined as the number of food groups eaten per day out of the following categories of food, with the priority outcome of interest being a minimum of 5 food groups per day:
Grains, white roots, tubers & plantains
Pulses
Nuts & seeds
Milk products
Meat, poultry & fish
Eggs
Dark green leafy veg.
Fruit & veg rich in Vitamin A
Other vegetables
Other fruits
Step 2: Identify the intended population
Given the context described in the previous section, and consultation with local stakeholders, the intended population for the segmentation analysis was pregnant women and mothers to children under 2 years of age.
Step 3: Enlist key stakeholders
For this segmentation effort, it was essential to engage key stakeholders in Mozambique including:
Members of the USAID Mozambique Mission
Members of the local Transform Nutrition project
Members of the USAID Advancing Nutrition project
Leaders of local NGOs (e.g. Feed the Change)
Step 4: Develop research questions
Based on a literature review and consultation with local stakeholders, several key research questions were developed, including those listed below.
Demographic factors
How many children do you have?
What is your marital status?
What is the highest level of education you have achieved?
Social norms
To what extent would you experience social consequences if you did not wait for your husband to eat?
Nutrition habits
What did you eat for breakfast yesterday?
What about after breakfast?
What did you eat for lunch? Anything else?
Agency and household dynamics
In your household, who makes the decisions about what food to buy?
What is the main barrier to accessing better food?
Knowledge and beliefs
What foods should a woman eat while pregnant? Why?
What messages have you heard about good nutrition while pregnant?
Emotions and feelings
How often do you feel lonely/isolated?
Figure 5. Thematic topics and examples of research questions, grouped into categories such as demographic factors, nutrition habits, knowledge and beliefs, social norms, agency and household dynamics, and emotions and feelings
Step 5: Select a dataset
In this example an existing dataset was not available, so primary research was conducted in Mozambique, first through a rapid test of a questionnaire and then a larger sample. The rapid testing was conducted among 100 pregnant women and mothers to children under two, using purposive sampling in four enumeration areas in Nampula.
Questions were then refined based on analysis of the smaller sample and a larger survey then launched with 300 women (pregnant or mothers of children under two) across 12 enumeration areas in Nampula, employing a randomized sampling approach to ensure the sample is as representative as possible.
Sample
Nampula
Pregnant women and mothers of children under 2
Phase 1: Rapid test
Initial questionnaire (~100 questions) administered to 100 respondents to identify early patterns and questions that had little variation in response. Following this analysis, the survey was revised
Purposive sampling
4 enumeration areas
N=100
Phase 2: Data collection
Updated questionnaire administered to a larger sample of 300 respondents to generate preliminary representative segmentation, identifying different groups of women with discrete dietary behaviors, beliefs, attitudes, and experiences of social norms.
Random sampling
12 enumeration areas
N=300
Figure 6. Description of quantitative research
Step 6: Define segments
Across the entire sample, there were some commonalities in behaviors and beliefs, notably:
Most women agreed that the ideal is to have three meals – breakfast, lunch, and dinner – not to feel hungry and to produce enough milk for the baby.
All women seemed to understand that a diverse diet is preferable.
Participants were unanimous on a good wife being a respectful woman, a woman who loves and respects her husband, and a woman who cares about family issues and takes proper care of the children.
Almost all participants agreed they share food with neighbors and friends, and they expect the same when in need.
Distinguishing Factors
The latent cluster segmentation analysis revealed four segments applicable to postpartum and pregnant women across Mozambique. The segments differ significantly with regards to dietary diversity, as well as 5 key factors. Flip the cards to learn about the 5 key factors.
Feelings of Social Connectedness
Social connectedness –
Does she feel socially connected to members of her community?
Household Decision-making
Household decision-making –
Is she an active participant in household decision-making?
Level of Anxiety Around Food
Level of anxiety around food –
How often does she feel anxious about food?
Barrier to Consuming Preferred Foods
Barrier to consuming preferred foods –
What is her main barrier to the food she wants?
Perceptions of Social Consequences
Social consequences –
Does she perceive her actions in regards to nutrition and food have social consequences?
Meet the Segments
This section summarizes the key characteristics of each of the segment personas identified among postpartum and pregnant women in Mozambique.
Laid-back Independent 19%
Illustrative summary
Confident, connected and autonomous women who can make better decisions regarding their dietary diversity
Social connectedness
Highly connected
Household decision-making
Makes the decisions
Level of anxiety around food
Rarely
Barrier to consuming preferred foods
Distance
Social consequences
Believes eating certain foods have social consequences, but still eats them
Busy Conscientious 33%
Illustrative summary
Busy women who have some decision-making power about their diet but are juggling many things
Social connectedness
Can feel isolated, meets people through her activities
Household decision-making
Decides with husband
Level of anxiety around food
Sometimes
Barrier to consuming preferred foods
Time
Social consequences
Cares about social perceptions
Satisfied Traditionalist 14%
Illustrative summary
Have little decision-making power about what food they grow, buy or eat and do not recognize need for better dietary diversity
Social connectedness
Connected to her small community
Household decision-making
Low autonomy and would like to be more involved
Level of anxiety around food
Sometimes/Rarely
Barrier to consuming preferred foods
Agency
Social consequences
Perceives few social consequences
Isolated Critic 34%
Illustrative summary
Somewhat isolated women who lack access to diverse food and decision making about what they grow, buy, or eat
Social connectedness
Isolated
Household decision-making
Can decide with husband, others are also involved
Level of anxiety around food
Often
Barrier to consuming preferred foods
Distance
Social consequences
Doesn’t care about social perceptions
Step 7: Refine segments
Additional qualitative research was conducted to further understand the nuances of the segments following the methodology described in the figure below. In total, 8 focus groups were conducted with 64 participants, lasting approximately 100 minutes per focus group discussion.
Topics discussed
Local context and cultural norms (e.g., attitudes and beliefs over what is a good diet, what a pregnant woman should eat, priorities of a wife/mother).
Important themes identified in quantitative analysis:
Social connectedness and activities undertaken with their community
Social norms (sharing food, community judgment)
Perceived barriers to dietary diversity
Anxiety/food insecurity
Specific questions about their segment
Differentiating characteristics uncovered in the qualitative analysis were explored for each segment
Data analyzed
8 focus groups (2 focus groups per segment)
64 participants (16 women per segment)
Participants from 6 communities (103 women identified per segment)
Women eating a maximum of 5/10 food groups
100 minute sessions
2 locations (Rapale and Mogovolas districts of Nampula)
Undertaken in local language Emakwa
Figure 7. Qualitative research methodology
This research helped uncover additional nuance regarding the main themes uncovered in the quantitative research, and how these differ by segment. For example, when examining social connection, the segments who reported more social connection in the quantitative survey (i.e., the Laid Back independents and Busy Conscientious segments) also discussed the importance of social connection during the qualitative focus groups. On the other hand, the Satisfied Traditionalist and Isolated Unaware segments described themselves as less social, and even expressed some judgment of other women who they consider to be overly social.
Representative Quotes
The following are quotes from the qualitative research, across the different segments regarding social connection. For more details on the research, download the final report.
Laid-back Independent
“When you are not friendly or don’t join other people, you get no idea to share with others.”
Busy Conscientious
“I belong to those who play much when I have time.”
Satisfied Traditionalist
“If you don’t have family nearby, you must look for a family in the same community you live in, that becomes your family.”
“We consider ourselves less social.”
Isolated Critic
“Sociable women […] leave their houses and go out to chat, drink, stay with others […] or can’t stay at home. […] You can easily notice that there is something wrong with them.”
After the segments have been refined and finalized, it is important to use a tool to identify segments in a given population. This is accomplished by identifying the most important questions to distinguish each segment (either through a qualitative assessment or advanced statistical analysis) and creating a simple and concise questionnaire to identify the segments with a high level of accuracy. For example, below you will find the segment identification tool that was developed based upon the dataset (N=300) of women in Nampula, which was further refined based upon the qualitative analysis.
Script for researcher or programmer: “Today, I will ask you a series of questions to help me understand the attitudes, behaviors and beliefs around nutrition of women during pregnancy and after they give birth. After I ask each question, I will state the answer choices. Choose the answer that best matches your experience and perception. I make no assumptions or judgments and want to hear from you on the following matters. There is no right or wrong answer.”
Segment Identification Tool Questionnaire
Question
Scorecard
Q1. When a woman is pregnant, what foods should she try to eat if she wants to stay healthy? (Record first answer they give)
Corn, wheat or starch [Proceed to Q2]
Fruits (not rich in Vitamin A) [Proceed to Q2]
Fruits rich in Vitamin A [Circle LI and proceed to Q3]
Meat (including organ meat) [Circle LI and proceed to Q3]
Local insects/animals [Circle BC and proceed to Q5]
Eggs [Circle BC and proceed to Q5]
Vegetables, dark green leaves or white roots [Ask “What else?”, and record new answer]
Other [Circle BC and proceed to Q5]
LI
BC
ST
IC
Q1. Scorecard
Q2. Most of the time, who decides what to eat every day? (if “Other”, choose who would be likely to make the decision between these 4)
My husband/partner [Circle ST and proceed to Q6]
Me [Circle IC and proceed to Q7]
Me and my husband/partner [Circle IC and proceed to Q7]
My mother/my mother-in-law [Circle IC and proceed to Q7]
LI
BC
ST
IC
Q2. Scorecard
Q3. Would you regularly eat more while pregnant?
I already regularly eat more when I am pregnant [Circle LI and proceed to Q5]
I would do it more if there were no social consequences [End interview]
No, I would not do that [End interview]
LI
BC
ST
IC
Q3. Scorecard
Q4. Do you regularly (at least once a week) participate in activities with people outside your household for entertainment or fun (watching soap operas together, playing, chatting where they sell alcohol, dancing)?
Yes [Circle LI and proceed to Q5]
No (I spend most of my time with my husband/children) [Proceed to Q5]
LI
BC
ST
IC
Q4. Scorecard
Q5. Besides cost, what prevents you from eating the foods you want to eat?
I am too busy/do not have time [Circle BC and end interview]
Other reason (for example: not available close to me) [End interview]
LI
BC
ST
IC
Q5. Scorecard
Q6. Most of the time, who in your household makes decisions on what you should eat while you’re pregnant or nursing?
My husband/partner [Circle LI and end interview]
Me [End interview]
Me and my husband/partner [End interview]
My mother/my mother-in-law [Circle ST and end interview]
Someone else [Circle ST and end interview]
LI
BC
ST
IC
Q6. Scorecard
Q7. In the past two weeks, how many times did you feel isolated or alone (lonely)?
Never [End interview]
Sometimes (1-7 days) [End interview]
Often (8-11 days) [Circle IC and end interview]
Every of almost every day [Circle IC and end interview]
LI
BC
ST
IC
Q7. Scorecard
Tally up the number of times each letter was circled. The letter with the highest number is the client’s segment.
LI
BC
ST
IC
__
__
__
__
Scorecard totals
Segment Codes
LI: Laid-back Independents
BC: Busy Conscientious
ST: Satisfied Traditionalists
IC: Isolated Critics
Using this tool allows SBC programmers, providers, or other stakeholders to identify client segments by asking a limited set of questions, with a high level of accuracy. Download the technical brief, Segmenting Nutritional Behaviors, for a printable version of the segment identification tool questionnaire.
In the next and final session, we will continue with this case example and discuss programmatic implications.
Key Takeaways
It is vital to start any segmentation process by identifying the nutrition-related priority behavior and clarifying the population of interest.
A segmentation process is best conducted by a team with diverse skills, experiences, and connections to the target population.
Review existing research on the intended population to gain a better understanding of what patterns and trends exist in the group, and what reasonable segments may look like. This background research will help inform the rest of the segmentation process, including developing research questions, determining the most viable segmentation model, and even brainstorming potential solutions.
While quantitative analysis helps uncover precise insights from existing data, qualitative research is beneficial for supplementing segment personas with a nuanced understanding of social and behavioral drivers.
A segment identification tool is created based on the key factors that differentiate the segments, to allow for a simple and effective way to identify which segment a person belongs to.
Check Your Understanding
Thank you for completing the second session of Audience Segmentation for Nutrition. Next is an ungraded quiz to test your understanding of Session 2. Click the Knowledge Check button to get started.
https://learning.breakthroughactionandresearch.org/wp-content/uploads/BA-logo-horizontal-300x110.png00Carriehttps://learning.breakthroughactionandresearch.org/wp-content/uploads/BA-logo-horizontal-300x110.pngCarrie2024-01-12 06:03:052024-03-30 16:33:44Case Study
The purpose of this session is to begin to describe how audience segmentation can be used in social and behavior change (SBC) programming for nutrition. This session describes the potential utility of audience segmentation to improve nutrition outcomes.
Learning Objectives
Define segmentation, demonstrate different types of segmentation, and provide a high-level overview of the steps to create a segmentation.
Describe how segmentation can be used to inform SBC programming.
Why Segmentation Matters for nutrition
Malnutrition remains a substantial global concern, and worldwide more than a quarter of children under five suffer from undernutrition. This includes 150 million children who are stunted or have a low height for their age, as well as more than 50 million who are wasted or have a low weight for their height, which can result from illness and undernutrition and are a major cause of child mortality. Undernutrition has a range of consequences that hinder social development, including leaving children vulnerable to disease, impoverishing families, diminishing community resilience, and reducing critical human capacity (USAID, n.d.).
However, nutrition is not only a concern for children. Poor nutrition of women and mothers affects both their health and that of their children, leading to higher rates of disabilities, mortality, stunted growth, disease predispositions, and low educational achievement (Rose et al., 2015).
As a result of these dynamics, USAID programs emphasize the “1,000 day window of opportunity” from pregnancy through a child’s second birthday, during which nutrition is critical for optimal physical and cognitive development (USAID, n.d.).
Additional Sources
FAO, IFAD, UNICEF, WFP, & WHO. (2022). The state of food security and nutrition in the world 2022: Repurposing food and agricultural policies to make healthy diets more affordable. https://doi.org/10.4060/cc0639en
Mothers gather for a nutrition program in Ahmedabad, India (Paula Bronstein/Getty Images/Images of Empowerment)
An Opportunity: The Role of SBC
While nutrition programming can be strengthened at a systems level, human behavior is also fundamental to improving nutrition outcomes. SBC initiatives are critical in addressing underlying social norms around nutrition and improving nutrition behaviors, using a range of approaches including targeted communication and social mobilization to ensure successful nutrition intervention outcomes. Several SBC nutrition tools can be found on the USAID Advancing Nutrition website.
To accelerate improvements in nutrition outcomes, segmentation analysis is extremely helpful for understanding the various factors, attitudes, and beliefs that influence nutrition-related behaviors. In doing so, segmentation can support SBC professionals in their strategy and program design efforts to ensure that they are tailoring their approach to reach those in need, and effectively encouraging positive nutrition-related behaviors.
What is Segmentation?
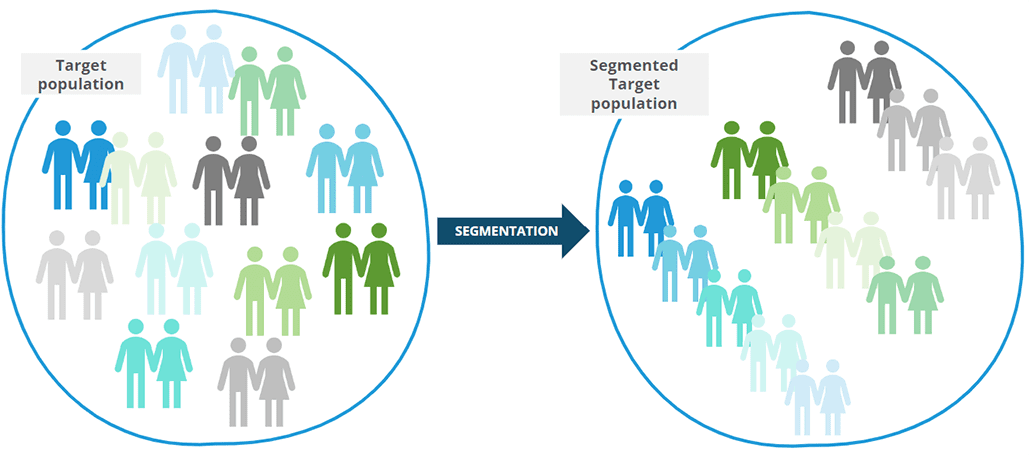
According to the Advanced Audience Segmentation for Social and Behavior Change How-to Guide, “segmentation divides a population or market into subgroups that have, or are perceived to have, meaningfully similar characteristics, and significant differences from other subgroups.” Figure 1 is a simple illustration of how segmentation can help us to understand a heterogenous population by organizing them into subgroups based on various factors and commonalities. In this illustrative example, they are grouped by colors; however, a segmentation analysis for nutrition might include segments with meaningful differences regarding dietary diversity, as highlighted in the case study presented in Session 2.
Figure 1. Visual representation of segmentation, sorting icons of blue, green, and grey people into groups by color
Segmentation allows for a nuanced look at a population and a deep understanding of what holds value for each group. This in-depth understanding can help stakeholders, such as national nutrition programs, community-based organizations, faith-based organizations, service delivery partners, private sector partners, and other implementing partners develop targeted SBC interventions and/or improve service delivery and increase the adoption of positive behaviors.
Below are definitions for two terms that will arise throughout the rest of this course.
Segment
A segment is a group of people with similar needs, values, or characteristics within a population, as identified through a segmentation analysis. Each segment has distinctive characteristics and is typically labeled with a name. Each segment has unique characteristics compared to other segments, meaning members within each segment are as similar to each other as possible, and as different as possible from other segments.
Segment Persona
A segment persona is a summary or description of the people who belong to each segment. It includes the key distinguishing factors that differentiate each segment and the most important drivers or barriers related to the desired social and behavior change(s). Segment personas help portray the segment as a real, tangible audience.
Types of Audience Segmentation
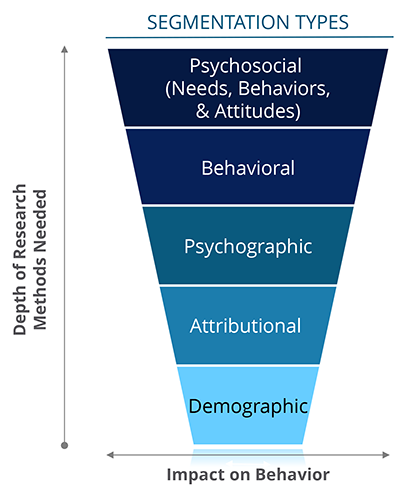
There are several types of audience segmentation: psychosocial, behavioral, psychographic, attributional, and demographic. Each type uses a different set of information to group a population into segments.
Psychosocial (needs, behaviors & attitudes)
Segmentation that identifies sub-groups within a population with different needs, attitudes, and willingness to change behavior. (optimal segmentationfor SBC programming)
Behavioral
Segmentation based on observable behavior, such as consumer activity or media use. This segmentation often relies on self-reported or observed behaviors related to the outcome variables. This type of segmentation reveals who is doing something, but does not help to understand why they are performing the behavior.
Psychographic
Segmentation based onbroad attitudes or personality traits, for example being “sporty” or a “foodie”.
Attributional
Segmentation based on a single attribute, such as life-stage, or property status. Single attribute segmentation can be based on variables beyond demographics, thus providing more interpersonal insights than demographic segmentation.
Demographic
Segmentation based on demographic factors, such as gender or age.
As illustrated in Figure 2, the simplest and most common method is demographic segmentation, which uses demographic data to create segments with different age groups, genders, or geographies. However, while individuals may be of the same demographic group, they likely still have significant differences with regards to their needs, beliefs and behaviors that would not be accounted for.
A more advanced audience segmentation method will be based on attributional,psychographic or behavioral variables, but will typically require more in-depth research to create the segments, which in turn can provide important insight into those segments’ potential for behavior change.
Figure 2. Segmentation types organized by depth of research methods needed and impact on behavior
Finally, a psychosocial segmentation (focusing on needs, behaviors, and attitudes) maximizes the opportunity for successful SBC and service delivery interventions. This type of segmentation can be used to understand the unique individual, social, and structural factors that influence the practice of the key behavior by members of the segment. Knowledge of the behavioral drivers that influence each segment can be leveraged to develop more tailored and effective SBC interventions for each segment.
To provide a very simple example of how this type of segmentation might show up in data, consider the following table with hypothetical data. (Note that steps to conducting a segmentation will be covered in more detail in Session 2, this is meant to provide an illustrative example.)
Performs positive health behavior (N=500)
Does NOT perform positive health behavior (N=500)
Women who believe X
85%
5%
Women who believe Y
5%
85%
Women influenced by Z
90%
10%
Table 1. Hypothetical illustrative example of analyzing data for segmentation
Based on the table above, we can see that women who “believe X” are significantly more likely to perform the positive health behavior. Women who “believe Y” are statistically more likely NOT to perform the positive health behavior and are less likely to be “influenced by Z”. Given the large sample size (N=500) for each column, these differences are statistically significant (meaning not due to chance).
In the case of nutrition, what this might look like is postpartum women who believe it is socially acceptable to eat certain vegetables (women who believe X) are more likely to eat the recommended number of food groups per day (performing the positive health behavior), whereas women who believe that preparing certain nutritious foods is too time consuming (women who believe Y) are less likely to eat the recommended number of food groups per day. And that women who trust health care providers for health information (women influenced by Z) are more likely to eat the recommended number of food groups per day. This is hypothetical data, but this example starts to lay out how data analysis leads to initial hypotheses regarding segmentation.
Overview of steps to create a segmentation
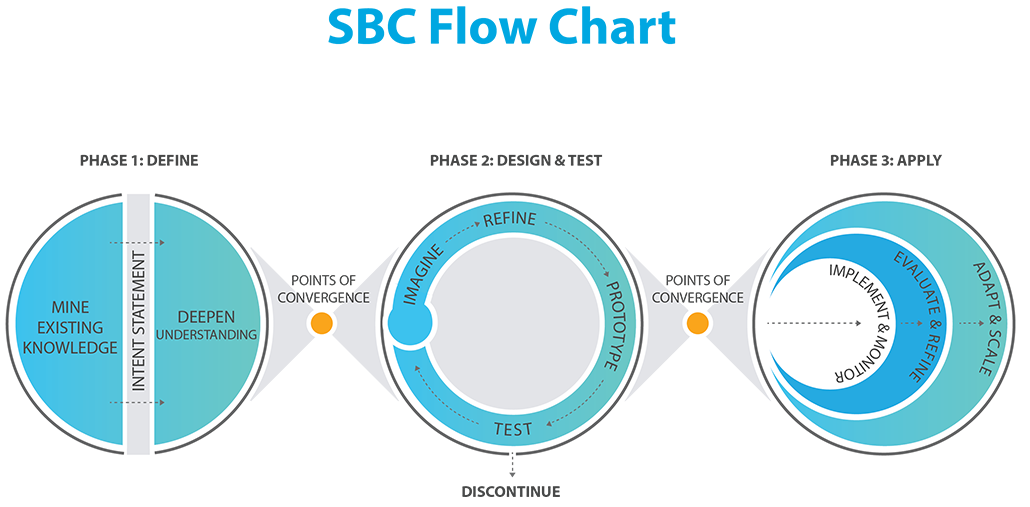
According to the Social and Behavior Change (SBC) Flow Chart, designed by Breakthrough ACTION, there are three main phases to developing effective SBC interventions while engaging end-users and stakeholders.
Figure 3. SBC Flow Chart
The steps for conducting a new audience segmentation can follow this phased structure to ensure a meaningful and thorough co-creation process. The following table provides more detail on these phases. The steps for audience segmentation will act as an outline for this session.
Description
Audience Segmentation Steps
Phase 1: Define and understand the problem
This phase assesses the findings and insights that already exist and establishes mechanisms to deepen understanding of the problem. This is accomplished by establishing relationships with those familiar with the subject of interest with whom to work with and uncover new perspectives and insights to guide solutions.
1. Identify the priority behaviors 2. Define the target population 3. Enlist key stakeholders 4. Develop research questions 5. Select a dataset 6. Define segments 7. Refine your segments
Phase 2: Design and test potential solutions and concepts
Grounded in deeper understanding, this phase informs how social and behavior change will be addressed by involving end users in the solution ideation process.
8. Develop intervention elements
Phase 3: Apply successful prototypes as activities or interventions
Once testing feedback has been synthesized into a prioritized suite of solutions, this phase marks their progressive implementation and evaluation.
Table 2. SBC Flowchart phases and corresponding steps for audience segmentation
We will cover these steps in greater detail in Session 2.
Leveraging Audience Segmentation
There are a number of ways that segmentation findings can be incorporated into the design of SBC interventions. Tailoring each aspect of an SBC intervention to the segment of interest can aid strategic resourcing for nutrition initiatives, helping to minimize redundancies and reduce inefficiencies in project design for maximum impact when limited resources are available.
For example, segmentation findings can be used in nutrition programs to:
Improve women’s and children’s food consumption behaviors and dietary diversity
Address specific breastfeeding mothers practices
Focus resources on groups with specific sanitation-related behaviors
Below are a few examples of SBC initiatives that can be developed with the use of segmentation analysis. Further detail on select nutrition SBC efforts developed with segmentation analysis will be described in Sessions 2 and 3.
CHILDREN Complementary Feeding
Feed with age-appropriate frequency, amount, and consistency
Feed children 6-23 months old a variety of age appropriate, safe, diverse nutrient-rich foods
Increase dietary diversity, consuming foods rich in micronutrients, energy, and protein
Ensure children continue to eat when ill
PREGNANT WOMEN Pregnancy & Breastfeeding Practices
Eat a variety of safe, diverse, nutrient-rich foods for meals and snacks daily while pregnant
Initiate breastfeeding within one hour after delivery
Breastfeed exclusively for six months or 180 days after birth
Continue breastfeeding until children are at least 2 years old
GENERAL POPULATION Sanitation-related Behaviors
Ensure optimal handwashing: wash hands with soap at critical moments
Encourage proper storage/treatment of water
Properly dispose of (adult, child, and animal) feces
Manage diarrhea at the onset of symptoms
Figure 4. Examples based on information from SBC technical guidance brief (USAID, 2017) and Infographic on behaviors to improve nutrition (USAID, 2020)
Key Takeaways
Malnutrition, particularly undernutrition in children, remains a critical global concern; SBC initiatives help reduce this burden by clarifying the role of human behavior in decision-making that affects nutrition.
Segmentation is a way to split a population into groups with similar characteristics. It can be used to develop more informed and tailored SBC programming.
A psychosocial (i.e. based on needs, behaviors, and attitudes) segmentation is best for understanding and encouraging behavior change, because it uncovers the root causes and underlying drivers of behavior.
Segmentation analysis can be leveraged for a wide variety of nutrition SBC efforts and topics.
Check Your Understanding
Thank you for completing the first session of Audience Segmentation for Nutrition. Next is an ungraded quiz to test your understanding of Session 1. Click the Knowledge Check button to get started.